Understanding mCSPC
Patients may present with, or progress to, mCSPC, which is rising in prevalence.
In a projection based on SEER data1:
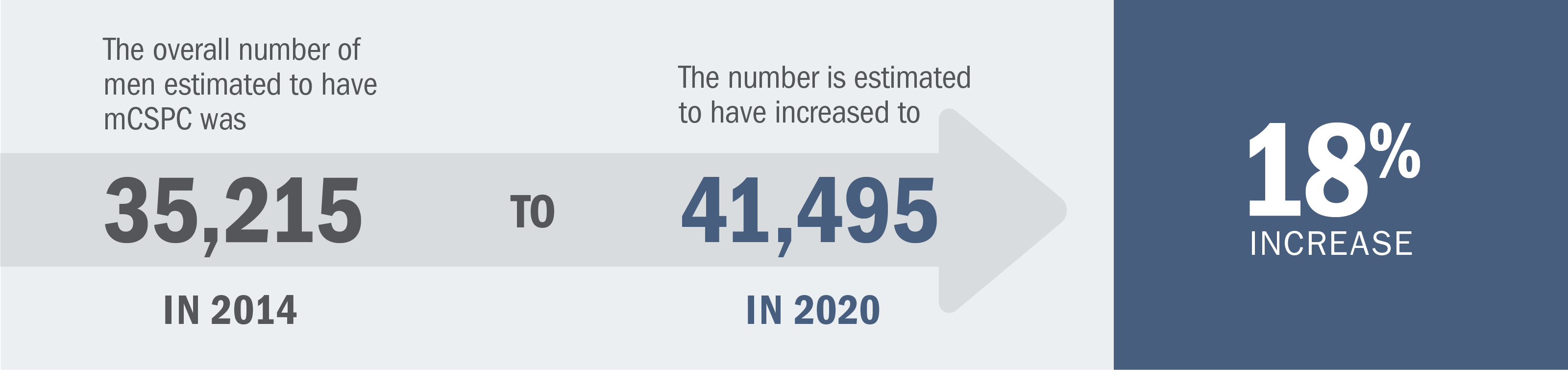
Based on a forward-looking model that used the Surveillance, Epidemiology and End Results (SEER) Program age-specific prostate cancer incidence rate data from 2008 to estimate prostate cancer incidence for each year from 2009 to 2020. To validate the model, the final results were compared with published estimates of prostate cancer incidence and prevalence in the United States for 2009 and 2020. The model estimates for the year 2020 are based on existing/current (2009) disease incidence, diagnosis, and treatment patterns, and reflect demographic changes in the US population over time (e.g., the impact of the baby boomer population).2
Patients with mCSPC can be diagnosed with one of the following:
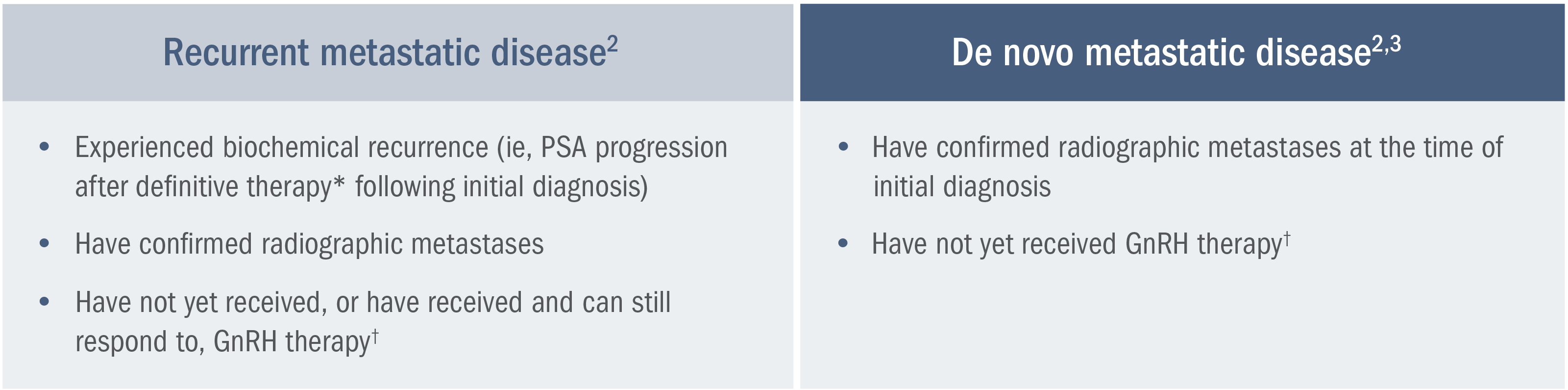
*Definitive therapy is defined as a radical prostatectomy or radiotherapy with curative intent.2
†Or after bilateral orchiectomy.2
Patients with de novo mCSPC are estimated to have a lower relative survival rate than patients with clinically localized disease.4
A SEER analysis* estimates a lower (37.9%) 5-year relative survival rate for patients with mCSPC vs those with clinically localized prostate cancer (100%).4
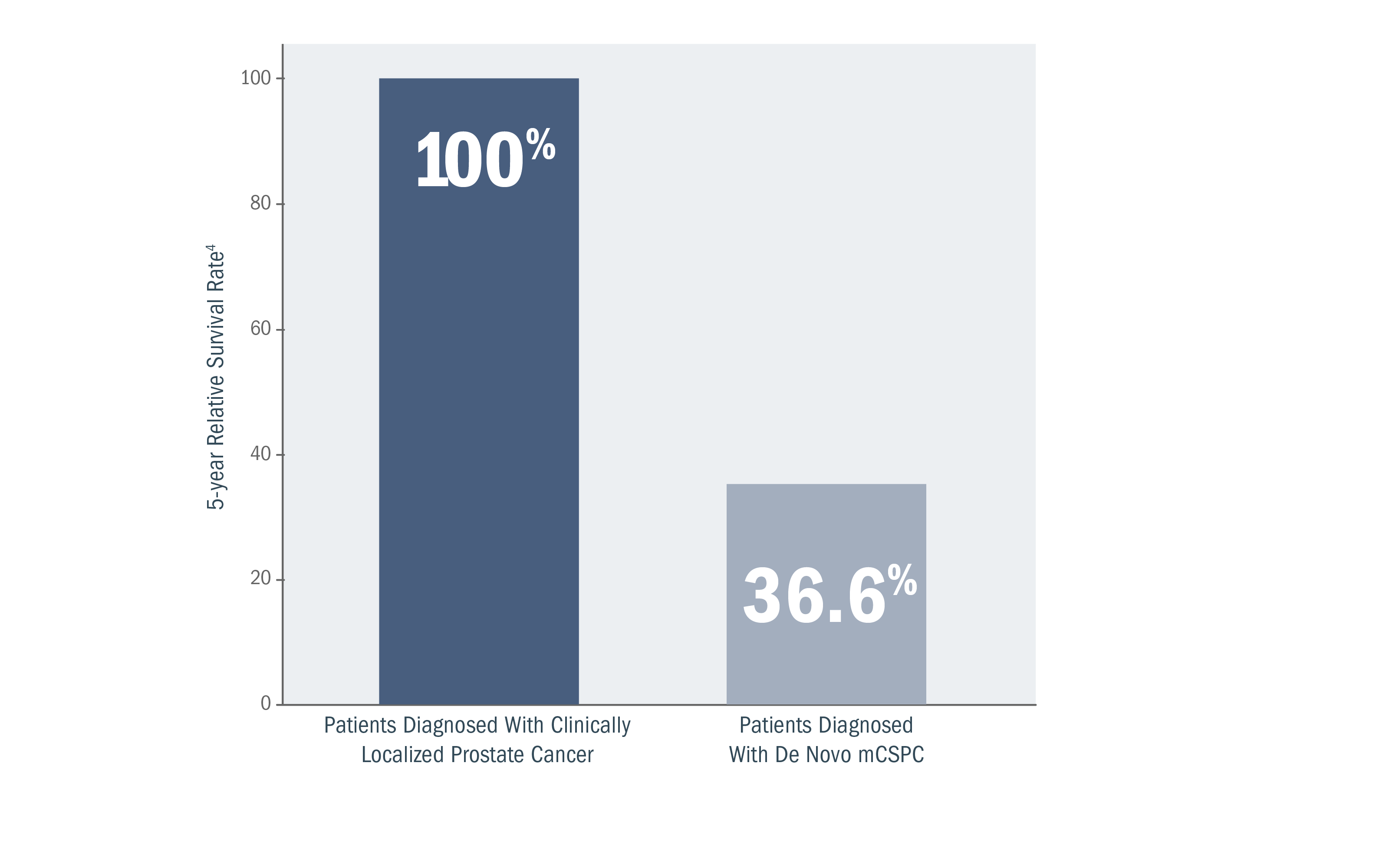
*A retrospective analysis of SEER database, a collection of cancer incidence and survival data from population-based cancer registries covering approximately 45.9%, per anchored support of the US population, was conducted between 2015 and 2021.4,5
Newly diagnosed mCSPC cases in the United States are projected to continue increasing.6,7
Annual projected (2020-2025) incidence of newly diagnosed mCSPC.6,7
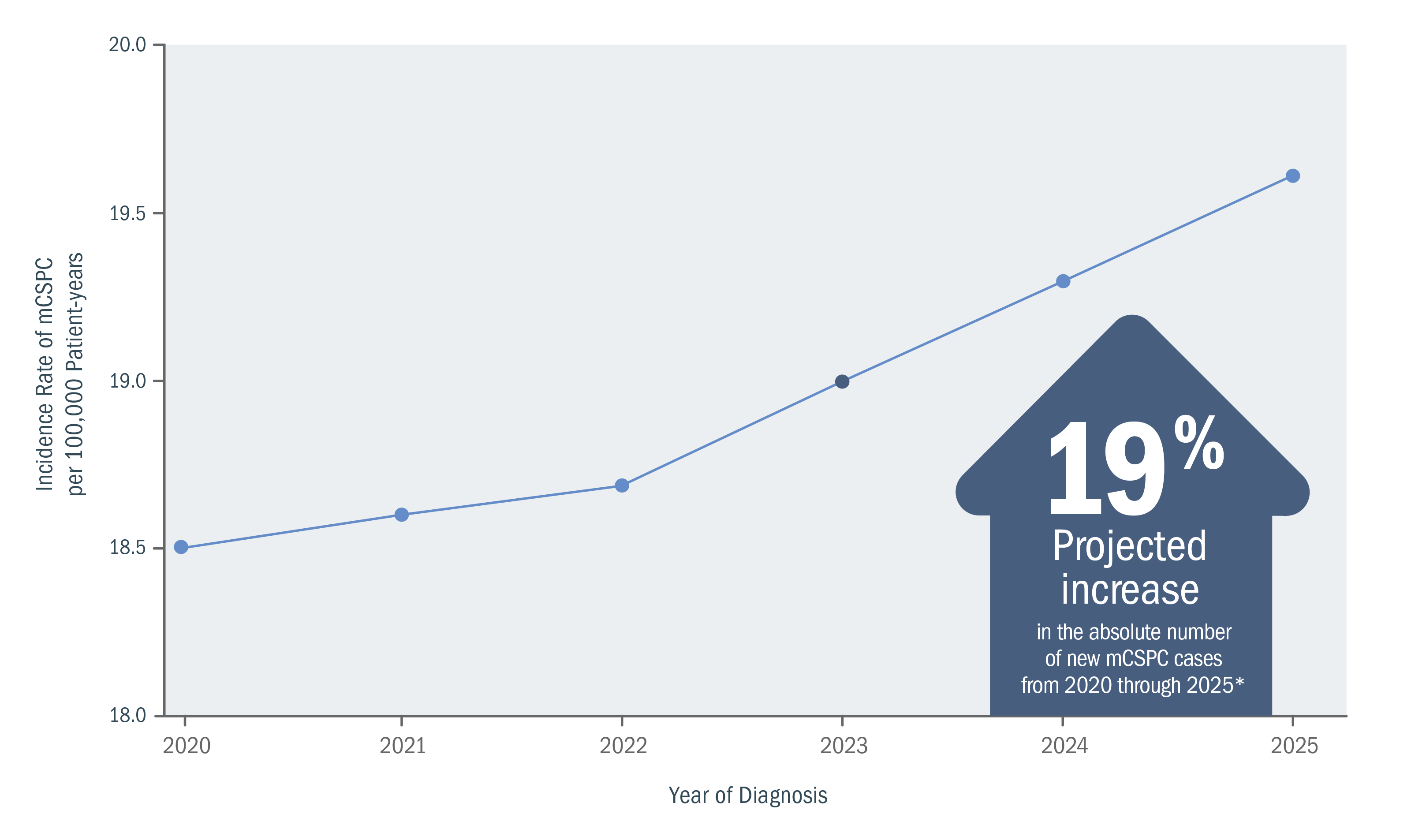
*From a 2018 study, based on age-period-cohort models and population projections of incidence data for men aged 45-94 years who were diagnosed with metastatic prostate cancer at initial clinical presentation. Estimates were based on the population-based SEER Program registries (2004-2014).6
Understanding the mechanism of disease (MOD) and implications in nmCSPC with high-risk BCR, mCSPC, and CRPC.
Mechanism of Disease
GnRH therapy and prostate cancer cell adaptation
In response to GnRH therapy, prostate cancer cells may adapt so that androgen receptor signaling continues to drive cell growth8-12

See how XTANDI may be able to help patients with mCSPC
View Trial ResultsUnderstanding nmCSPC with biochemical recurrence (BCR) at high risk for metastasis
Risk for metastasis remains even after definitive therapy.*1,2
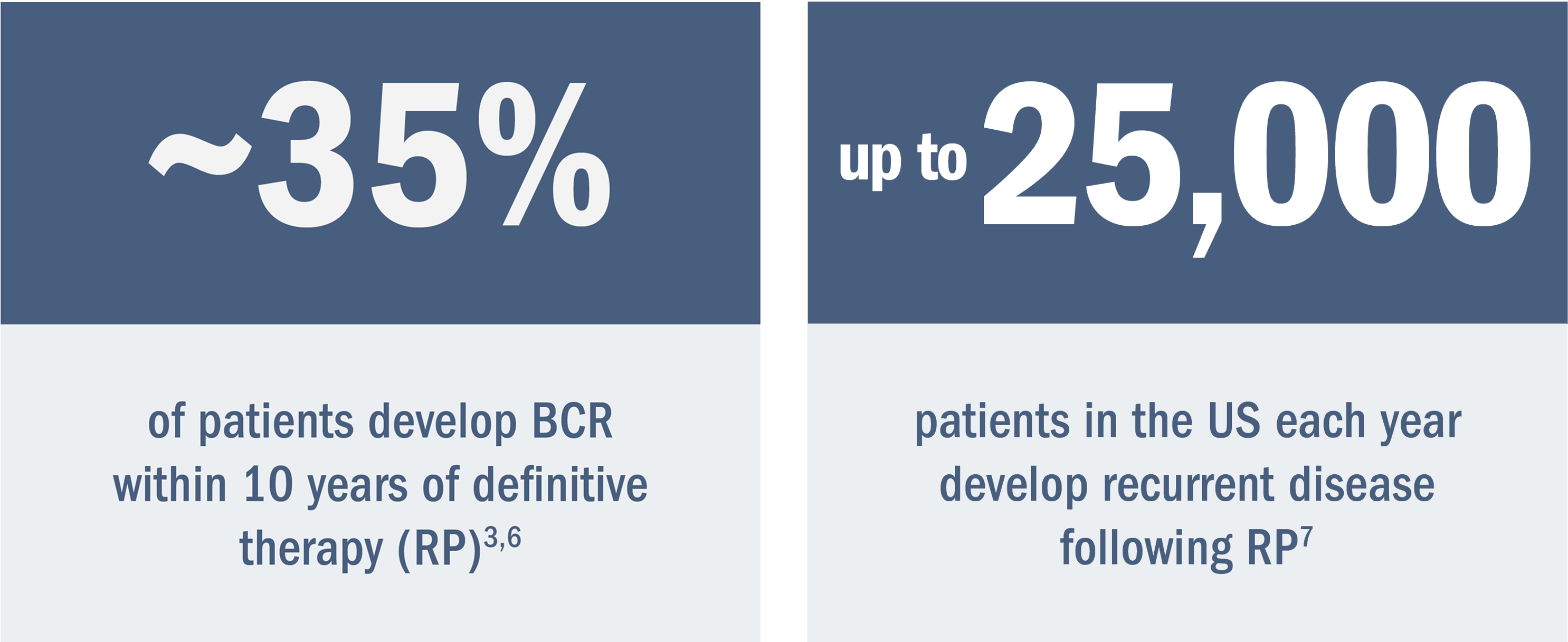
Some men may develop metastasis after definitive local therapy with radical prostatectomy (RP) or radiation (RT).1,2
*Treatment for localized disease.
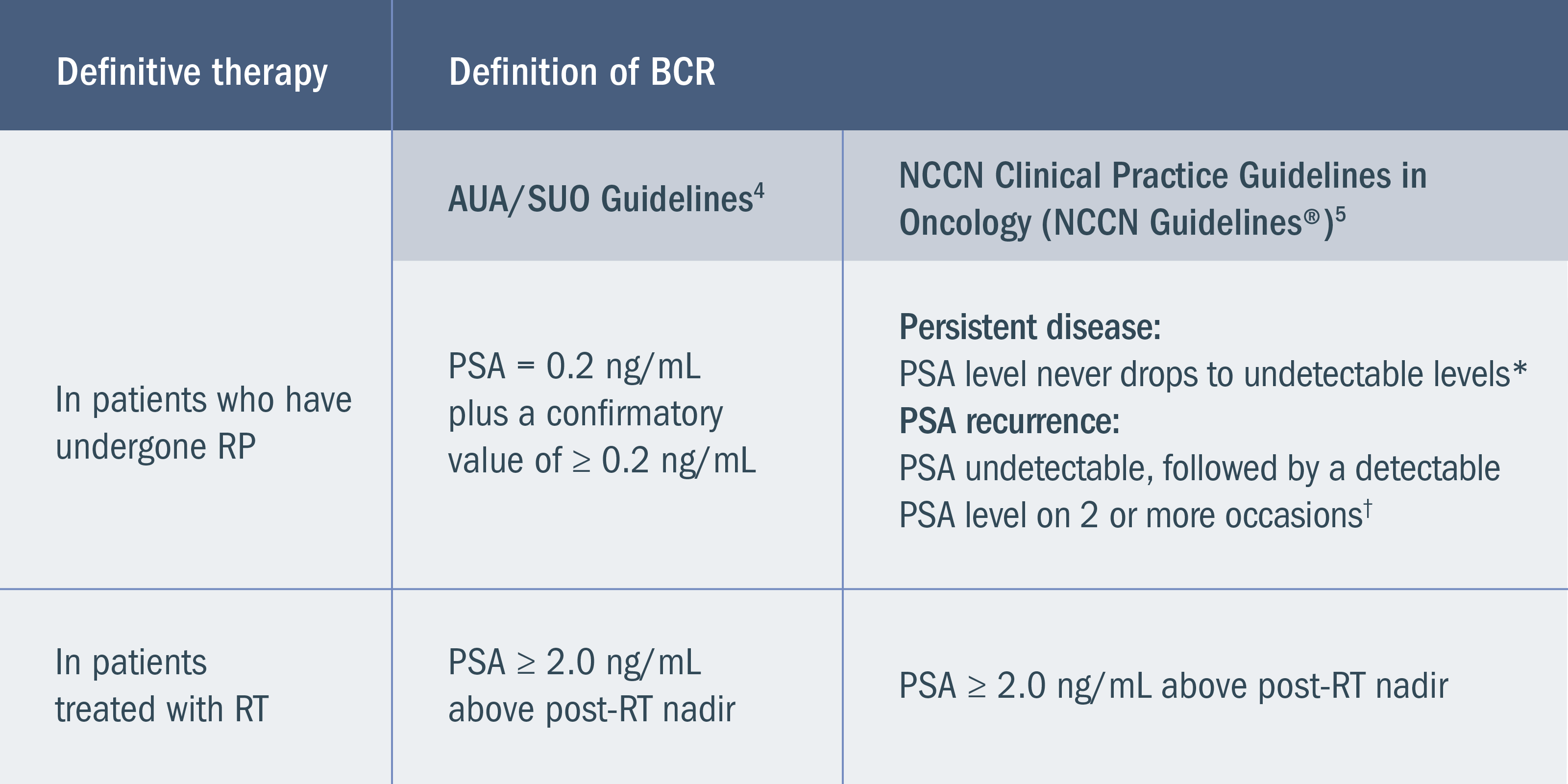
BCR is defined by rising PSA without macroscopically detectable disease after the failure of definitive therapy.4
BCR may occur in patients who do not have symptoms. The definition of BCR is based on the type of prior definitive therapy, and guidelines vary slightly between the National Comprehensive Cancer Network® (NCCN®) and American Urological Association (AUA)/Society of Urologic Oncology (SUO)4,5:
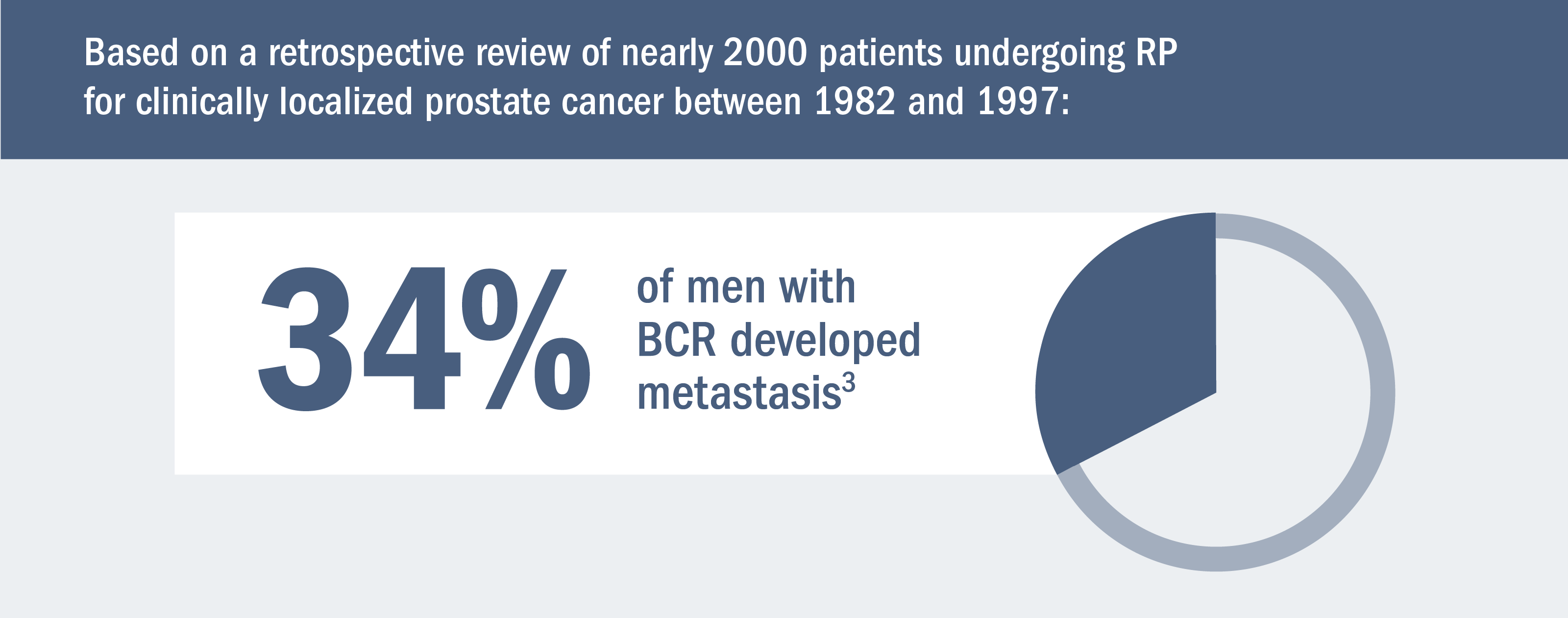
Based on 2 retrospective studies (n = 1997 and n = 304) as well as estimates of men with preoperative high-risk disease, rates of RP, and rates of BCR3,6,7:
Shorter PSA doubling time is associated with increased risk for metastasis.4,6,8
At the time of BCR in nmCSPC, PSA doubling time has been shown to be one of the most reliable indicators of the risk for further disease progression. A PSA doubling time of < 9 months has been associated with poor prognosis.8-10
Based on a retrospective analysis of men treated with RP at a single hospital6,8:
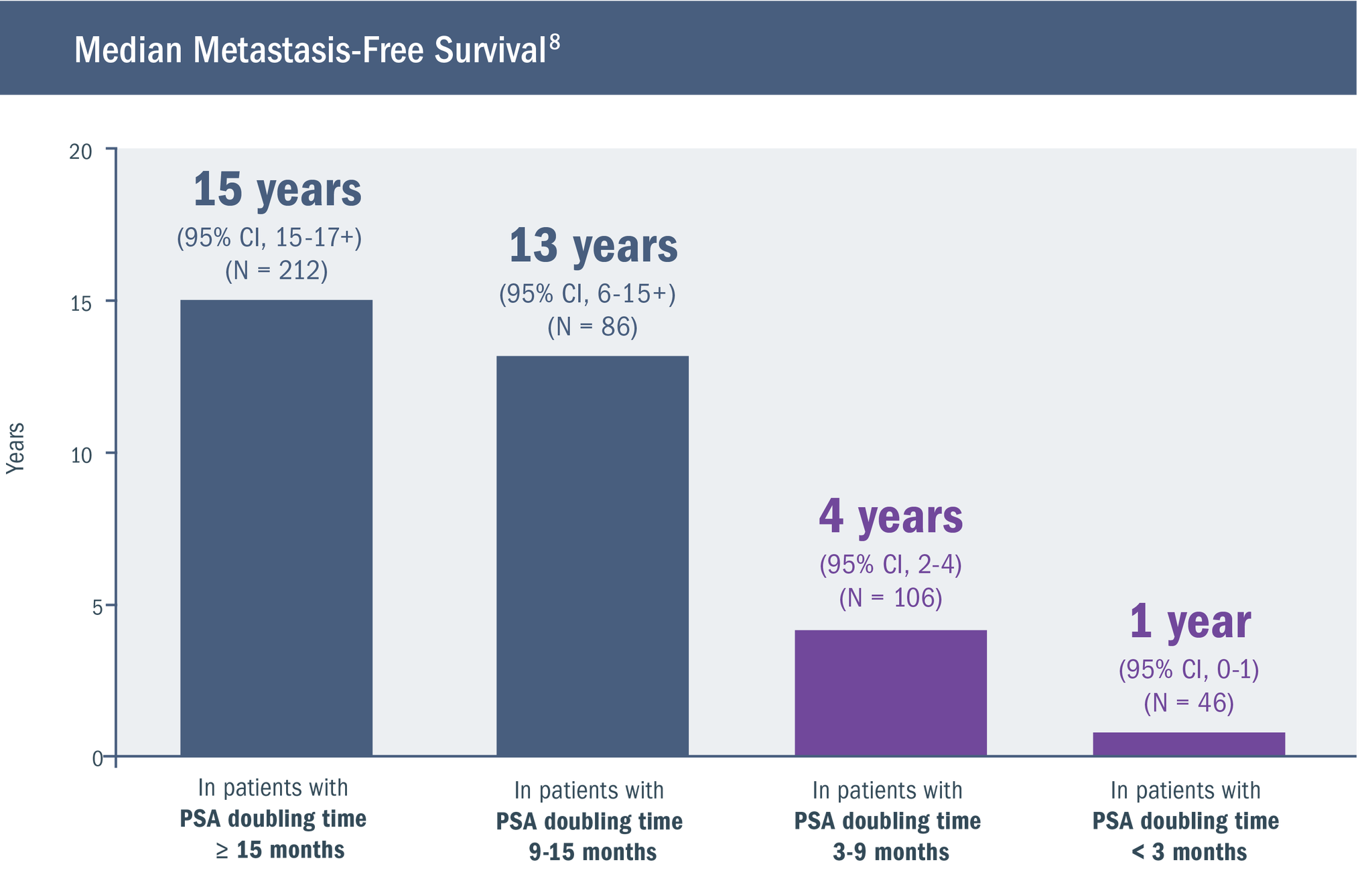
- While patients with local recurrence have a PSA doubling time of 13 months, those with a PSA doubling time of 3 months present with distant metastases11
- The number of patients in the above study was relatively small, requiring that the findings be viewed as preliminary8
Watch a video in which Dr. Jason Efstathiou discusses the impact of high-risk BCR on prostate cancer prognosis.

Identifying patients with nmCSPC with high-risk BCR is an early step in prognosis and guiding the management approach3,14
Guidelines recommend monitoring PSA levels after definitive treatment.5
Following treatment with curative intent for localized prostate cancer, serial PSA measurements with clinical evaluation can be important during follow-up. These measurements enable the determination of PSA doubling time, which is a reliable indicator of the risk for disease progression.4-6,9,10
The options recommended for PSA testing by the NCCN Guidelines® for Prostate Cancer are5:
Patients at high risk of recurrence:
Every 3 months
Other patients: Every 6 to 12 months
The NCCN Guidelines suggest the option of considering tumor stage, Gleason score, and initial PSA when determining if a patient is at high risk of recurrence.5
In this video, Dr. Daniel Petrylak discusses monitoring patients for high-risk BCR.
See Dr. Evan Goldfischer review profiles of 3 hypothetical patients with high-risk BCR
Understanding the mechanism of disease (MOD) and implications in nmCSPC with high-risk BCR, mCSPC, and CRPC.
Mechanism of Disease
GnRH therapy and prostate cancer cell adaptation
In response to GnRH therapy, prostate cancer cells may adapt so that androgen receptor signaling continues to drive cell growth.15-19

See how XTANDI may be able to help patients with nmCSPC with high-risk BCR
View Trial ResultsCRPC, castration-resistant prostate cancer; CSPC, castration-sensitive prostate cancer; GnRH, gonadotropin-releasing hormone; mCSPC, metastatic castration-sensitive prostate cancer; nmCSPC, nonmetastatic castration-sensitive prostate cancer; PSA, prostate-specific antigen.