
View and download useful resources about XTANDI for your office
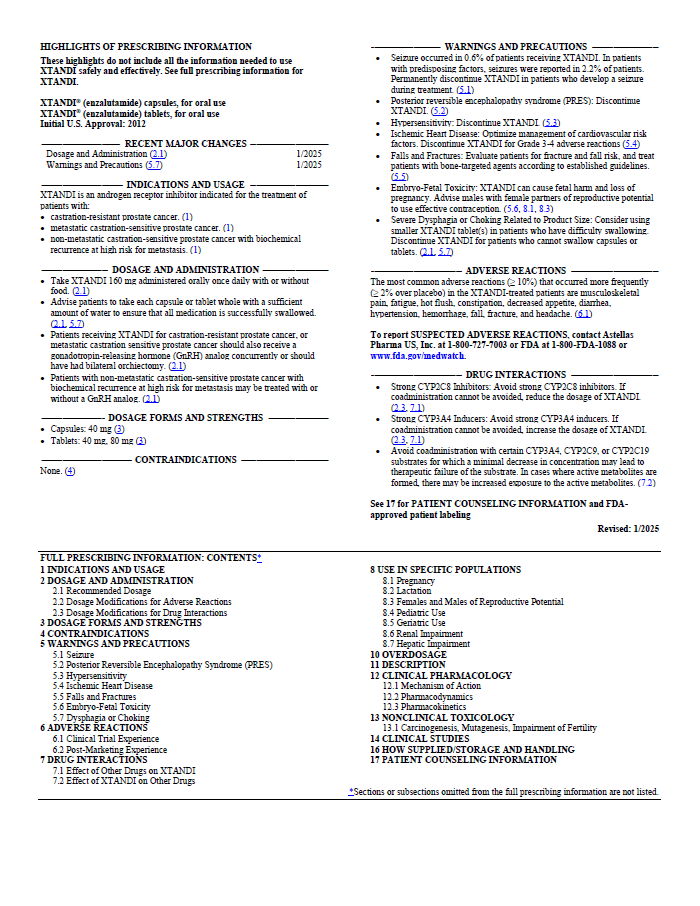
US Full Prescribing Information for XTANDI,
Including Efficacy, Safety, and Dosing
Get information about XTANDI.
View & Download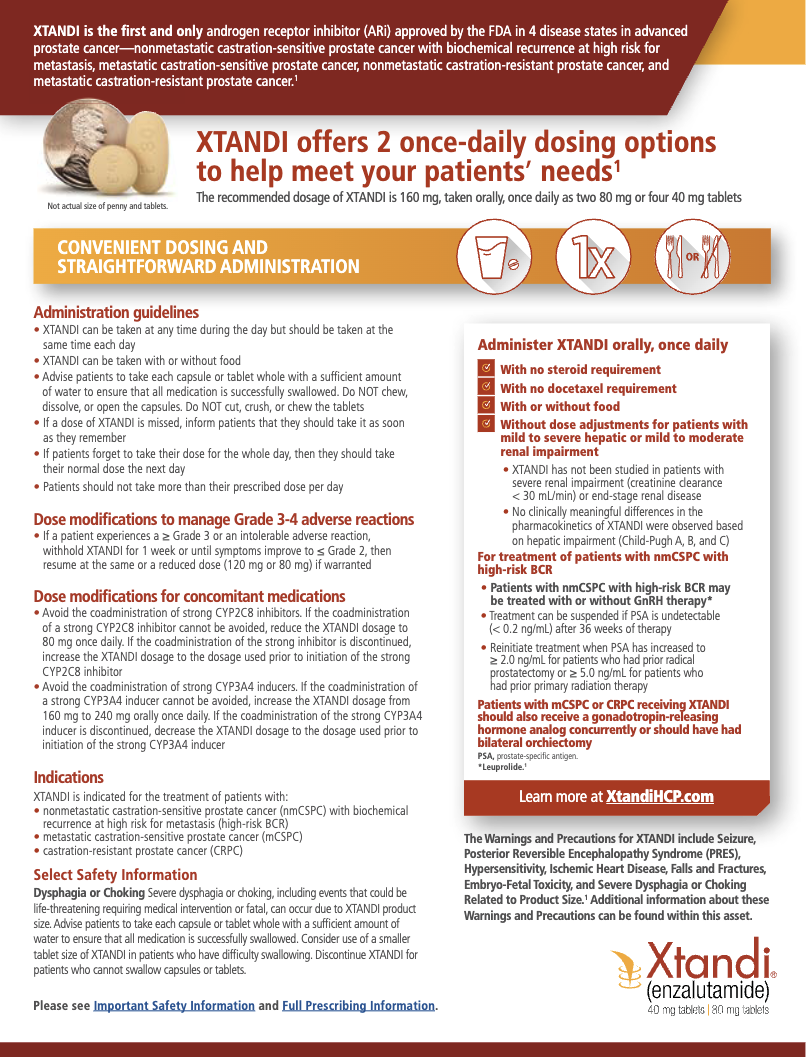
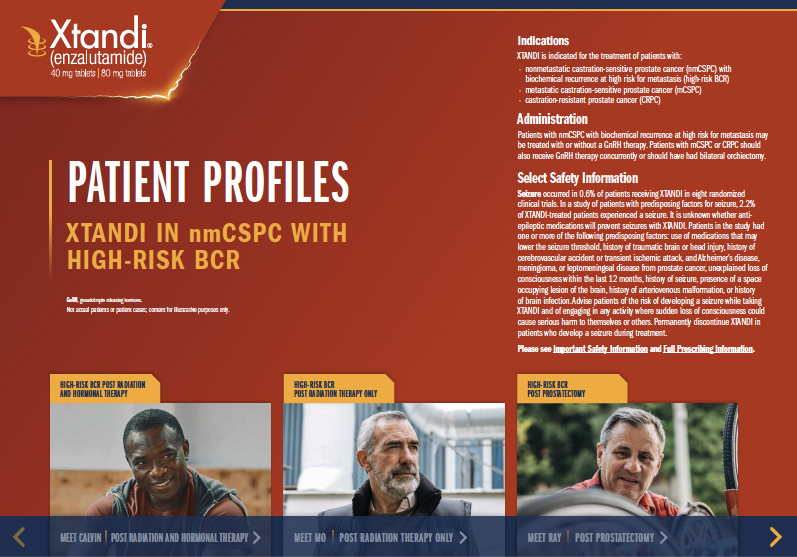
nmCSPC With High-Risk BCR Patient Profiles Brochure
Explore profiles of patients with nmCSPC with high-risk BCR who are eligible for XTANDI.
Not actual patients or patient cases; content for illustrative purposes only.
mCSPC Patient Profiles Brochure
Explore profiles of patients with mCSPC who are eligible for XTANDI.
Not actual patients or patient cases; content is for illustrative purposes only.
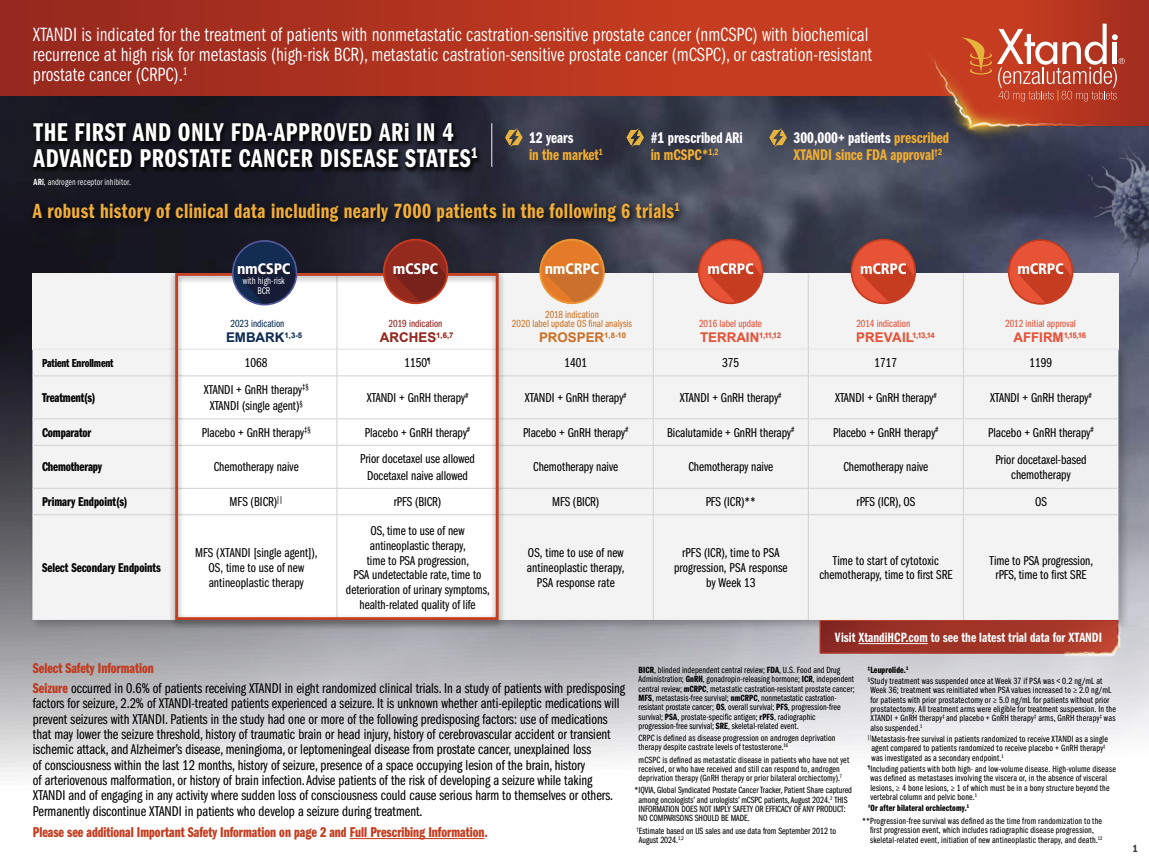
XTANDI Heritage Flashcard
Take a closer look at the details of 6 clinical trials that resulted in XTANDI label updates.
View & Download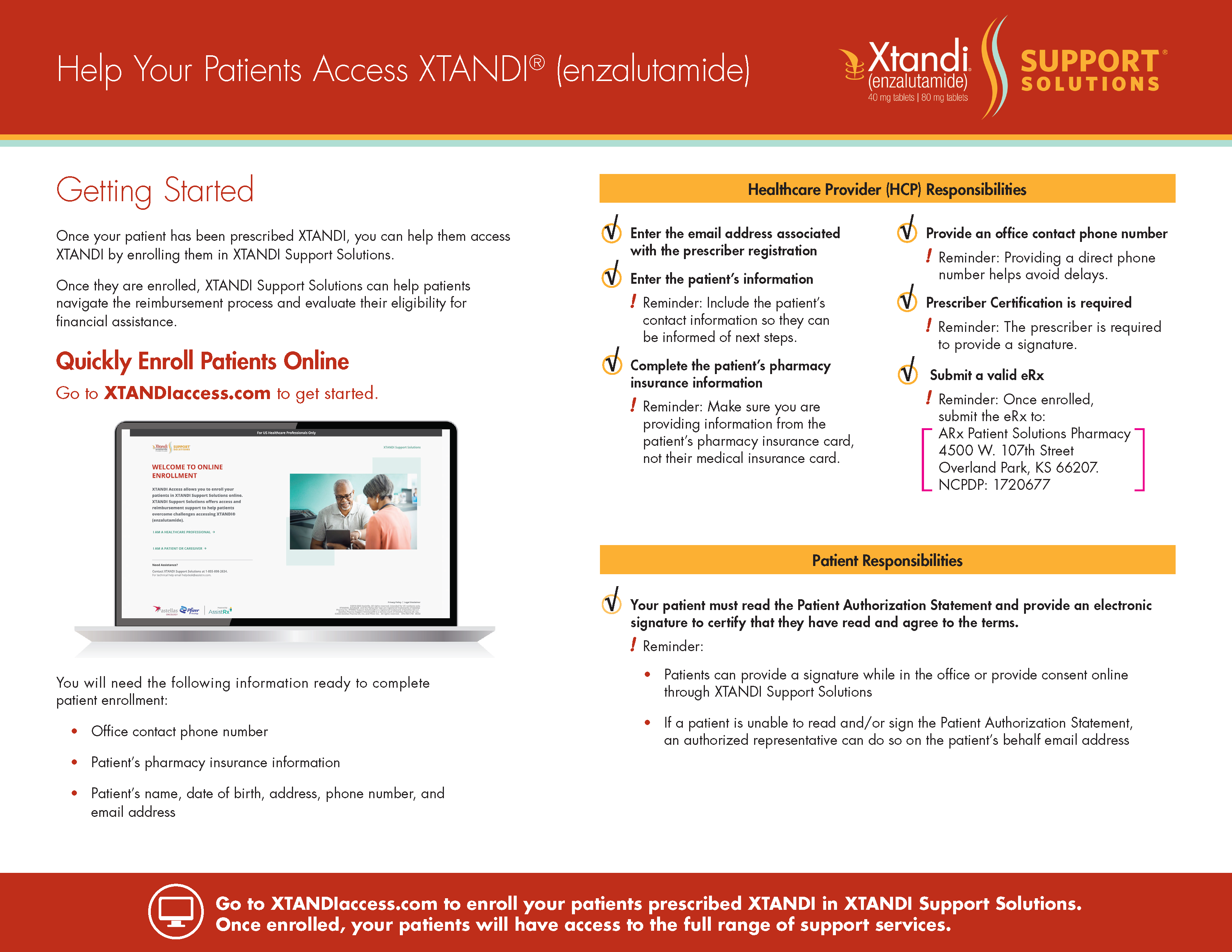
Getting Started with XTANDIaccess.com
Find information to help your patients enroll in XTANDI Support Solutions.
View & DownloadExplore publications that report clinical trial data for XTANDI
Freedland SJ, de Almeida Luz M, De Giorgi U, et al. Improved outcomes with enzalutamide in biochemically recurrent prostate cancer. N Engl J Med. 2023;389(16):1453-1465. doi:10.1056/NEJMoa2303974.
Go To PublicationShore ND, de Almeida Luz M, De Giorgi U, et al. Improved survival with enzalutamide in biochemically recurrent prostate cancer [published online ahead of print October 19, 2025]. N Engl J Med. 2025. Accessed October 20, 2025. https://www.nejm.org/doi/full/10.1056/nejmoa2510310.
Go To PublicationArmstrong AJ, Szmulewitz RZ, Petrylak DP, et al. ARCHES: a randomized, phase III study of androgen deprivation therapy with enzalutamide or placebo in men with metastatic hormone-sensitive prostate cancer. J Clin Oncol. 2019;37(32):2974-2986. doi:10.1200/JCO.19.00799.
Go To PublicationArmstrong AJ, Azad AA, Iguchi T, et al. Improved survival with enzalutamide in patients with metastatic hormone-sensitive prostate cancer. J Clin Oncol. 2022;40(15):1616-1622. doi:10.1200/JCO.22.00193.
Go To PublicationArmstrong AJ, Petrylak DP, Shore ND, et al. ARCHES 5-year survival with enzalutamide plus androgen-deprivation therapy in metastatic hormone-sensitive prostate cancer patients [published online ahead of print February 3, 2026]. Eur Urol. 2026. Accessed February 19, 2026. https://www.sciencedirect.com/science/article/pii/S0302283825048766?via%3Dihub.
Go To PublicationHussain M, Fizazi K, Saad F, et al. Enzalutamide in men with nonmetastatic, castration-resistant prostate cancer. N Engl J Med. 2018;378(26):2465-2474. doi:10.1056/NEJMoa1800536.
Go To PublicationSternberg CN, Fizazi K, Saad F, et al. Enzalutamide and survival in nonmetastatic, castration-resistant prostate cancer. N Engl J Med. 2020;382(23):2197-2206. doi:10.1056/NEJMoa2003892.
Go To PublicationPREVAIL
Beer TM, Armstrong AJ, Rathkopf D, et al. Enzalutamide in men with chemotherapy-naïve metastatic castration-resistant prostate cancer: extended analysis of the phase 3 PREVAIL study. Eur Urol. 2017;71(2):151-154. doi:10.1016/j.eururo.2016.07.032.
Go To PublicationTERRAIN
Shore ND, Chowdhury S, Villers A, et al. Efficacy and safety of enzalutamide versus bicalutamide for patients with metastatic prostate cancer (TERRAIN): a randomised, double-blind, phase 2 study. Lancet Oncol. 2016;17(2):153-163. doi:10.1016/S1470-2045(15)00518-5.
Go To PublicationAFFIRM
Scher HI, Fizazi K, Saad F, et al. Increased survival with enzalutamide in prostate cancer after chemotherapy. N Engl J Med. 2012;367(13):1187-1197. doi:10.1056/NEJMoa1207506.
Go To PublicationDownload useful resources about XTANDI to share with your patients
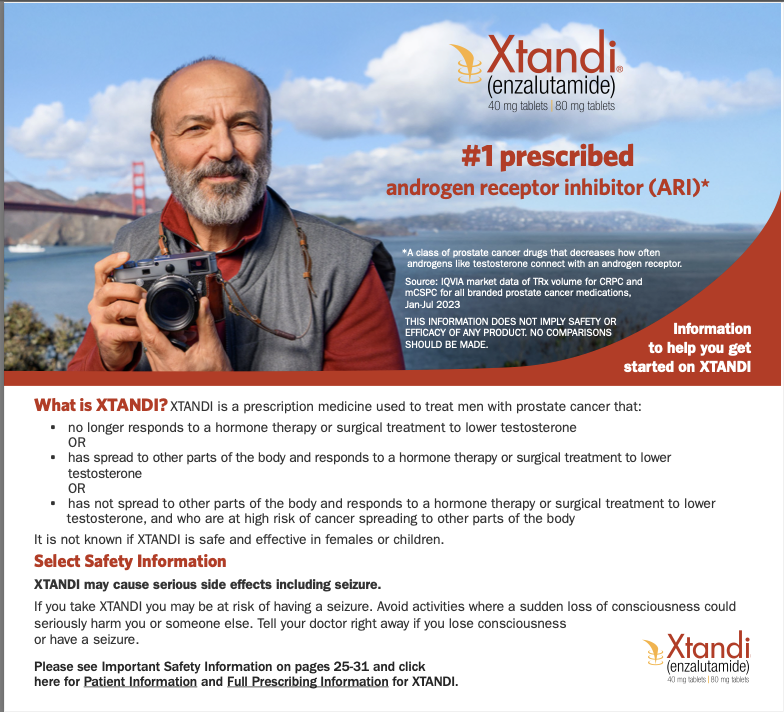
Getting Started Brochure
This resource provides patients with information about XTANDI and advanced prostate cancer.
View & Download
Questions for Patients to Ask Their Doctor
Patients can use this guide to prepare for their next doctor visit.
View & Download
Side Effects Overview for Patients
Share this overview with your patients to help them learn about the potential side effects of XTANDI.
View & Download
XTANDI Support Solutions® Pamphlet
Patients can learn about XTANDI Support Solutions and get support.
View & Download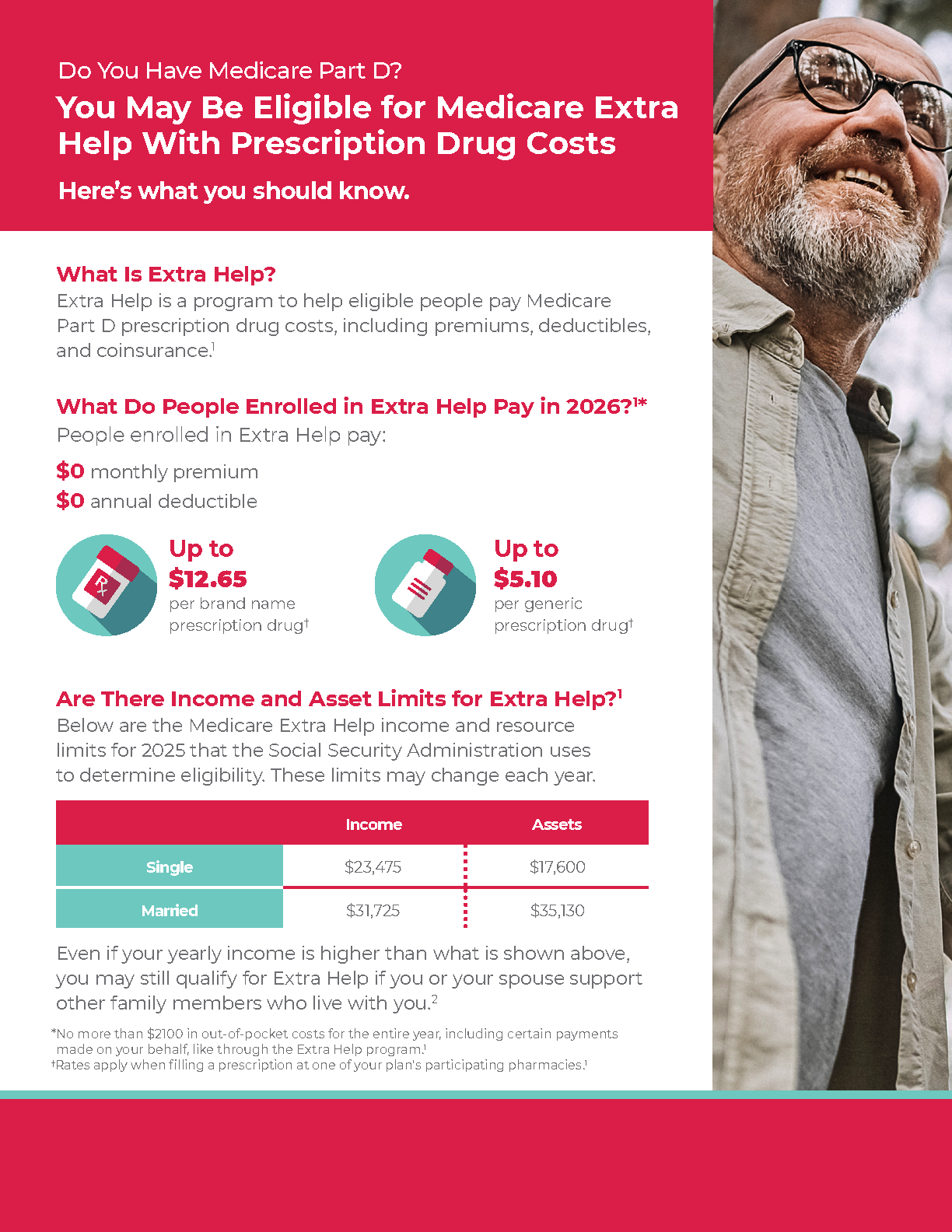
Medicare Extra Help Patient Flashcard
Extra Help is a program to help eligible people pay Medicare Part D prescription drug costs, including premiums, deductibles, and coinsurance.
View & Download (English) View & Download (Spanish)Links to patient support organizations
The organizations listed here offer a variety of services that include support, information, and advice to help your patients learn about living with prostate cancer.
Astellas and Pfizer are not affiliated with, do not own or control, and are not responsible for the content or services contained on the websites. The information provided by Astellas and Pfizer is for informational purposes only and is not meant to replace a doctor’s or nurse’s advice.
PATIENTS GET
STARTED
ON XTANDI
GET STARTED ON XTANDI
Or call 1-855-8XTANDI
(1-855-898-2634)
Monday–Friday, 8 AM–8 PM ET